
QUATTROFIX IMPLANT-SUPPORTED FIXED PROSTHESIS IN PATİENT WITH PROGRESSIVE PERIODONTAL DISEASE
Patient History
A 46 years-old female patient with progressive periodontal destruction with poor oral hygiene was evaluated by panoramic X-ray and intraorally. There were deep (>6mm) infected periodontal pockets and intense smoking in the patient who did not have enough motivation to maintain oral hygiene with the present teeth. Due to the periodontal disease all teeth have severe bone loss and mobility which can not promise long-term success. In the light of these circumstances, extraction of all teeth and treatment with quattrofix implant system in both jaws with immediate loading was planned. Because the patient had long upper lip, no bone reduction need was planned preoperatively. After extraction of the teeth, implants were placed and immediate loading with PMMA temporaries was performed for a three months healing period. After the healing period, permanent metal ceramic prostheses were delivered. Because the patient has metal-ceramic restorations in both jaws and patient indicates that she is bruxist, a hard occlusal splint was also fabricated to protect the proshteses from any parafunctional habit. Patient has also quit smoking and gained her oral hygiene motivation back in the end of the treatment.

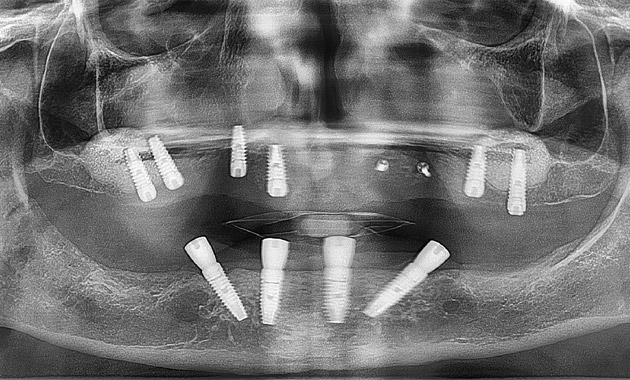
#1 Preoperative panoramic radiography showing severe bone loss due to periodontal disease and poor oral hygiene

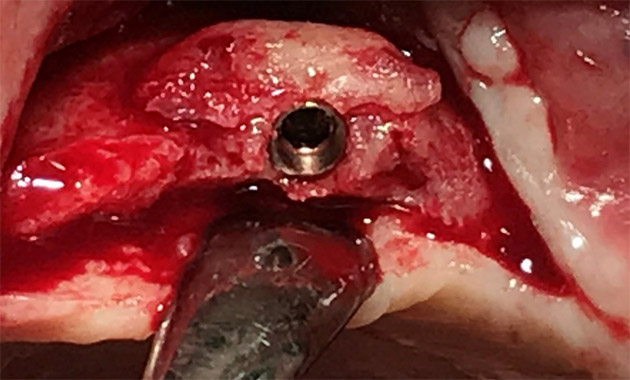
#2 Placement of multiunit healing caps after extractions, placement of implants and multiunit abutments.

#3 Placement of multiunit healing caps after extractions, placement of implants and multiunit abutments.

#4 Immediate PMMA temporaries produced by Cad-Cam
Quattrofix Implant System
Quattrofix implant system is a treatment protocol to enable the use of fixed implant supported prosthesis in severe atrophy of the jaws by avioding further bone grafting procedures, increased costs and morbidities (1).
System offers immediately loading of implants placed in anterior regions of both jaws and reaches up to to 1st molars. Anterior two implants are placed axially while posterior two implants are placed titled with an angle varying between 17 to 45 degrees. Thanks to tilted implants, distal cantilever length is reduced and 12 teeth per jaws can be placed on the prosthesis which can increase chewing function efficacy (2,3)
This treatment protocol has short and mid-term success in the literature and offers a fast and efficient solution for the patients. So it has widely been performed among dentists to rehabilitate these kind of severely atrophic jaws (4).

#5 Open tray multiunit impression copings are placed in both jaws for impression of permanent prosthesis at 3rd month
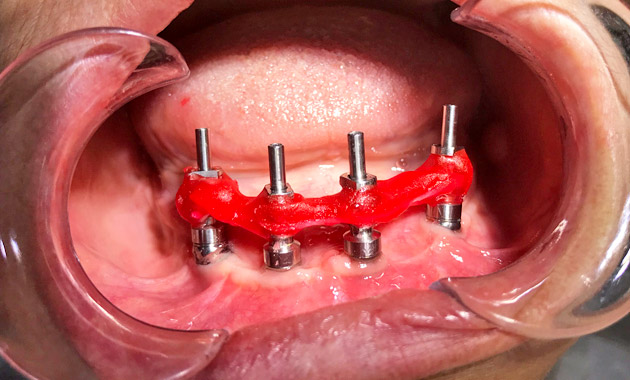
#6 Pattern resin material is used to take an accurate impression for a passively fitting restoration

#7 Passive adaptation was checked for each screw at control session of screw retained metal base
Surgical Considerations in Quattrofix Implant System
- Long implants are used in patients with low quality bone to get anchorage from cortical areas such as nasal floor, lateral wall of maxillary sinüs.
- 35Ncm primary stability of the implants is aimed. If this value is not being reached, immediate loading should be avoided.
- A minimum of 5 mm width and 10 mm length of bone between intercanine area is required in edentulous maxilla.
- A minimum of 5 mm width and 8 mm length of bone between intercanine area is required in edentulous mandible.
- A thorough curettage in extraction sockets should be performed to avoid residual lesions.
- Distal implants should be tilted up to 45 degrees to minimize cantilever length.
- Distal implants should be placed first, then anterior implants should be placed.
- Occlusal screw holes of the posterior implants should arise from occlusal schemes of 1st molar, 2nd premolar or 1nd premolar.

#8 Porcelain fused metal restorations were checked on account of gingival adaptation, cleanbility and passive fit and delivered to the patient

#9 Porcelain fused metal restorations were checked on account of gingival adaptation, cleanbility and passive fit and delivered to the patient
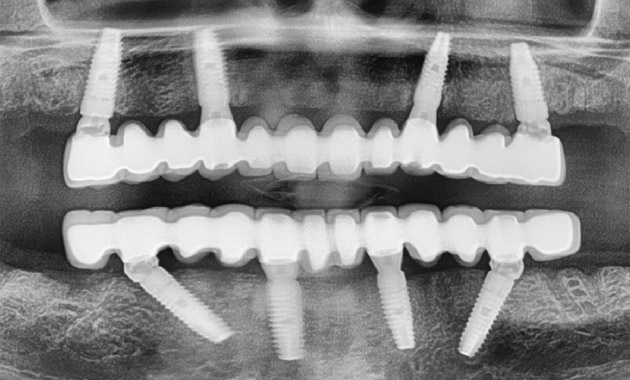
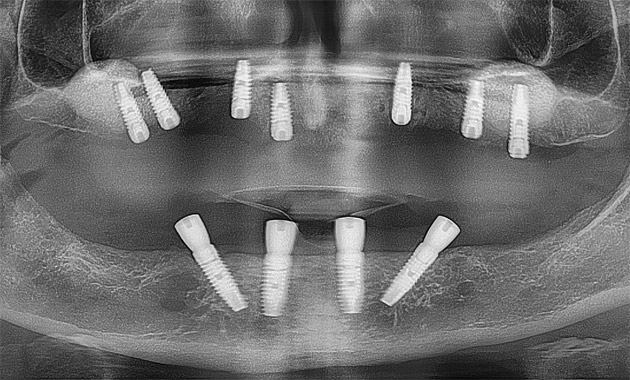
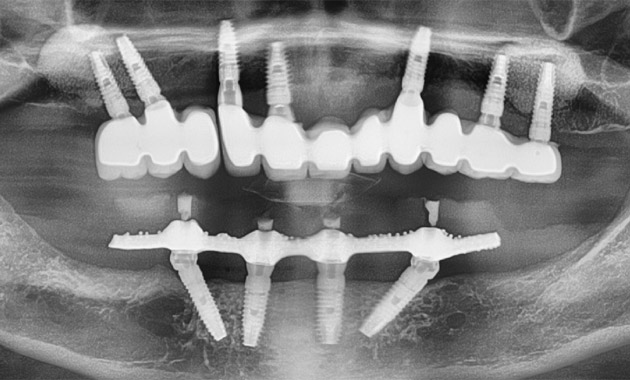
#10 Post-operative control radiograph
BILATERAL SINUS LIFTING, AUTOGENOUS BONE GRAFTING AND IMPLANT TREATMENT TO REVISE A FAILED IMPLANT TREATMENT

#1 Pre-operative panoramic radiograph shows severe periodontal destruction around lower teeth and thin posterior alveolar ridge was presenting a knife-edge apperance.
#2 Conventional implant treatment in maxilla with bilateral sinus lifting, autogenous ramus graft was performed while quattro-fix system was applied in mandible. Immediate loading was not performed in both jaws and healing abutments were placed prior to implant placement in lower jaw.
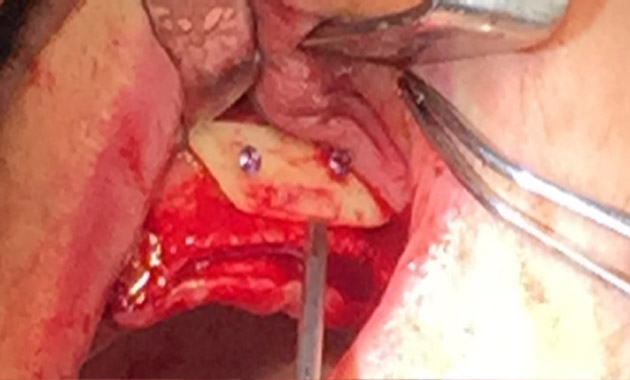
#3 Autogenous ramus bone graft for gaining bone in horizontal direction at canine region was performed and tissue was closed in a tension-free fashion.
#4 At the end of 4th month autogenous bone graft area was opened and fixation screws were removed. Implant was placed subsequently to the regenerated bone. Despite the periphery of the block graft was a little bit resorbed, it became possible to place the implant supported by surrounding bone.
Autogenous bone grafts are the gold standard in bone augmentation procedures by having osteoinductive and osteogenesis mechanisms. By having these properties, autogenous bone grafts are superior to alloplastic and allogenic materials in cases that need regeneration (1,2). Ramus area is the mostly used region which offers a minimal invasive approach option, lower donor site morbidity, patient discomfort. The bone graft is harvested from external oblique ridge of ascending ramus mandible. Separation of the autogenous ramus bone graft material to horizontal layers which is also known as Khoury technique is among the most successful and mostly used methods (3,4).
#5 Postoperative panoramic x-ray image 3 months after the last implant was placed. After a 7 months of healing period, healing abutments in maxilla and multiunit abutments in mandible were placed. Porcelain fused metal bridge in maxilla and hybrid prosthesis by using metal based acrylic in mandible was planned. Open tray impressions by using pattern resin was performed in both jaws that enabled us to deliver a perfect impression to laboratory.
#6 Open tray impression copings placed on multiunit abutments and connection of copings with pattern resin material. After cutting the connection areas of pattern resin between neighbouring copings, the gaps were filled with pattern resin again which eliminates shrinkage of polimerisation of pattern resin and prosthetic problems arising of it.

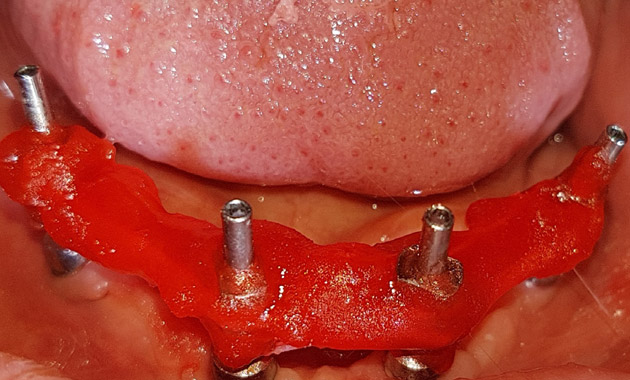
#7 Passive fit of the bar which will be hidden in the quattrofix prosthesis was checked in the mouth. Laboratory was informed for keeping the distal cantilever not more than 10 mm.

#8 Delivery of quattro-fix implant prosthesis. Angled multiunit abutments and prosthetic screws were tightened with 15Ncm, while straight multiunit abutments were tightened with 25Ncm. Prosthetic screw holes were closed with teflon band and composite resin.
Patient History
A 65 years-old woman patient without any systemic disease was referred to our clinic with complaint of pus and pain on her previously placed implants in another center. There were deep, inflammed periimplant pockets and a severe halitosis. Her CBCT scan revealed severe bone loss on buccal walls of all implants and poor implant angulations. Extraction of all of the implants and residual teeth, horizontal bone augmentation with an autogenous ramus graft, bilateral sinus lifting in maxilla and all on four in mandible was planned.

#9 Abutments in maxilla were placed and tightened with 25Ncm.

#10 Postoperative view after delivery of the prostheses.
#11 No bone loss was observed at the postoperative 1st year follow-up panoramic X-ray radiograph.