
REHABILITATION OF TOTAL EDENTULISM BY DENTAL IMPLANTS AND SINUS LIFTING
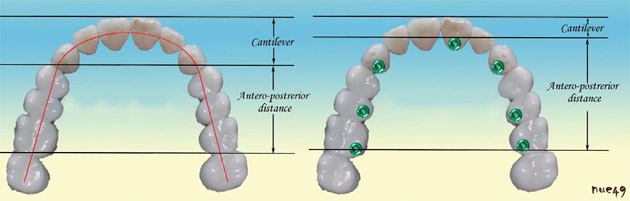
#1 Implant planning in ovoid arch formed maxilla
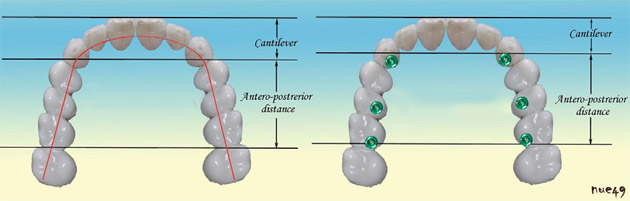
#2 Implant planning in ovoid arch formed maxilla
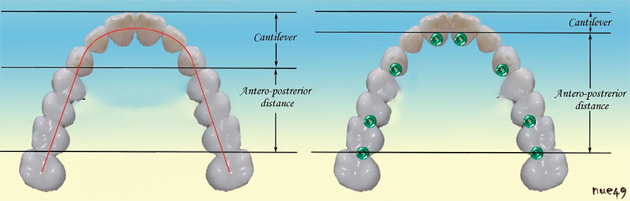
#3 Implant planning in anteriorly narrowing maxilla
Planning of an implant-supported fixed prosthesis may require different numbers and placement of implants due to theanatomy of maxillary and mandibuar bones. Six implants are mostly considered as enough in mandible, while there may be more implants to be placed in maxilla due to the spongious bone structure. Type of maxillary arch is crucial to determine the appropriate number of implants in maxillary implant placement. (1,2)
Ovoid Total Edentulous Maxilla
In this type of maxillary arch, a minimum of seven implants are suggested. The location of implants are, one in central or lateral incisor region, bilateral canines, bilateral second premolars and bilateral distal part of first molars. The prostesis is recommended to be splinted for balanced force distrubution. If the clinician suspects any signs of heavy occlusal force or parafunction, an additional anterior implant and bilateral second molar implants will help to increase antero-posterior distance.(3)
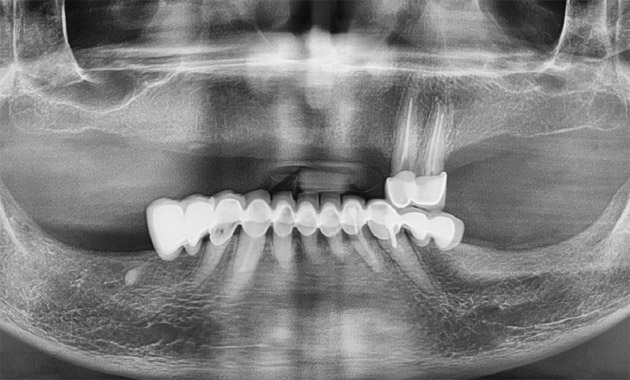
#4 Pre-operative OPTG shows bone loss around teeth

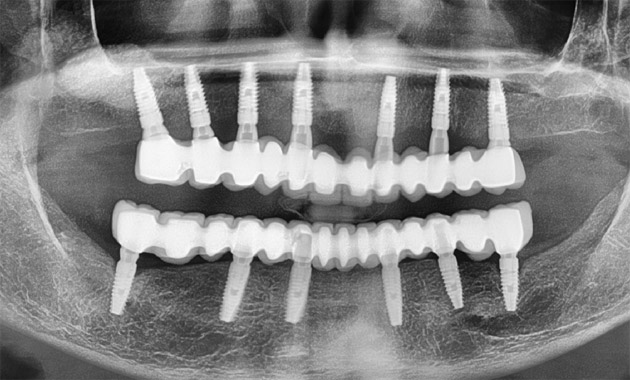
#5 Tooth extractions, implant placements and direct sinus lifting on right side was performed simultaneously. Due to the ovoid arch form of maxillary alveolar bone, seven implants were placed in the maxilla while six implants were sufficient in mandible when cortical bony structrure was taken into consideration

#6 Intraoral view of abutments before cementation of the prosthesis. No temporary prosthesis have been used during the three months of osseointegration period
Square Total Edentulous Maxilla
The minimum number of implants is six in this type of arch. Bilateral canine, bilateral second premolars and bilateral first molars are the appropriate implant placement regions
Anteriorly Narrowing Edentulous Maxilla
If the maxillary arch is narrowing in anterior direction, the minimum implant number has to be eight. Additional implants are placed in central or lateral teeth regions in premaxilla.
The number of implants to be placed in maxilla depends on anatomy of maxillary arch and bone density. If there is low-quality bone, increased number of implants will increase bone implant contact surface and antero-posterior distance (4)

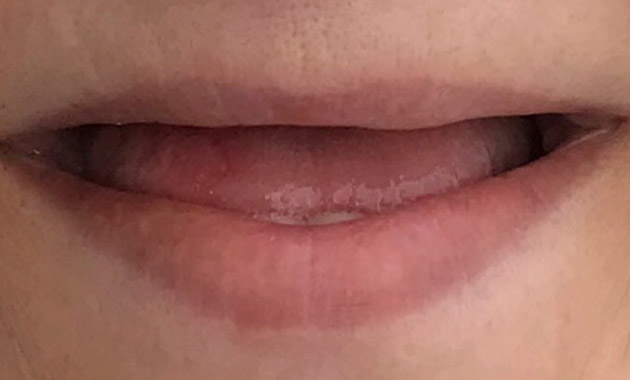
#7 The extraoral view of patient without teeth and with her teeth prosthetic in try-in appointment. Midline, low smile line were some of the paramenters that were checked in this session

#8 Prosthesis was cemented and the aesthetic result was satisfactory
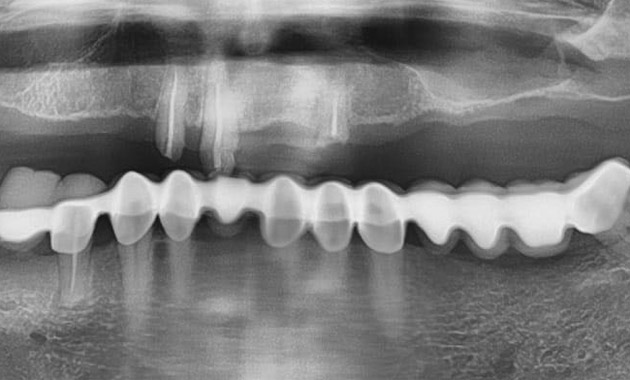
#9 One year follow-up OPTG shows no bone loss. Oral hygiene motivation was assured and annual follow-up sessions were recommended to the patient
Case Presentation
A 40-year-old female patient who presented no sistemic disease demanded fixed prosthesis and implant treatment. Intense smoking habit (two packages in a day), chronic periodontitis, severe tooth mobility, infected periodontal pockets, bone loss in both horizontal and vertical dimensions were observed. Tooth extractions, oral hygiene motivation and implant-supported fixed prosthesis was planned.
KEY PROSTHETIC FACTORS IN PATIENTS TREATED WITH QUATTROFIX SYSTEM
Patient History
A 58 years-old female patient without any systemic disease was referred to our clinic for fixed prosthesis demand. Heavy smoking habit was present and patient was informed about potential risks of smoking on our treatment success. Her maxilla was severlely resorbed and primary suggestions were bone augmentation or zygomatic implants. The patient refused these further surgeries and a quattro-fix implant system with a short occlusion was offered as the last alternative and she accepted this plan. Bone reduction requirement was pre-operatively evaluated carefully which was having a great importance at this case to achieve aesthetics by hiding the finish line of the proshtesis under the lip. The implants were immediately loaded by a temporary proshtesis and after three months, metal-ceramic prosthesis ending at first molars are fabricated and delivered to the patient.
Smile Line
Patients present three types of smile lines as follows: High, moderate, low smile line. The most advantageous patient profile is the ones who present small mouth and long upper lip. It’s easier to achieve aesthetics in these patients. The patients with high smile line may have aesthetic problems if not taken into consideration on account of lip line. The finishing margin of the proshthesis. Planning the finish line of quattrofix prosthesis under the smile line before the surgical operation is crucial. The need for bone reduction especially in patients presenting high smile line should be carefully taken into consideration. Another key point is evaluation of the smile line before injection of local anesthesia or patient’s preoperative photographs showing the face. (1,2,3)
#1 Preoperative radiograph showing the excessive bone loss in posterior maxillary regions
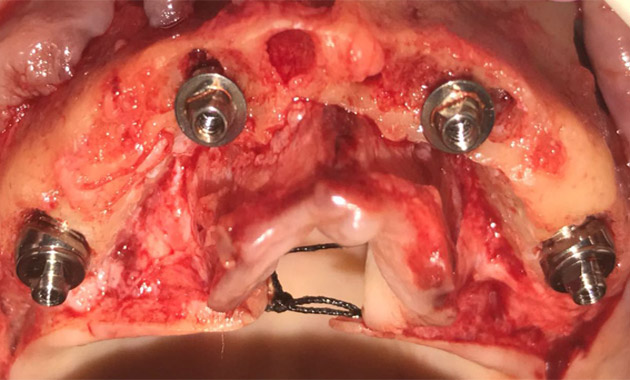
#2 After the extraction of the residual roots, bone reduction for achieving aesthetics was also performed. Multiunit abutments are tightened to the immediately placed implants
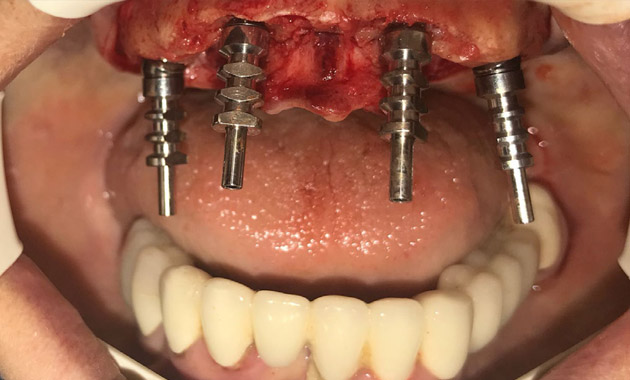
#3 Open tray multiunit impression copings placed and intraoperatively impression was taken for temporary prosthesis
Lip Support
Bone resorption progress from anterior to posterior in maxilla which causes pseudoprognatism in totally edentulous patients. The need for lip support and the connection angle of the prosthesis to tissues are related to each other. When the need for lip support is too much, bone reduction may also be required even though the finish line of the proshtesis is under the lip which offers a more cleanable proshtesis with a reasonable emergence profile from the tissues. So the interarch relations are essential to evaluate preoperatively (4).
Parafunction
Bruxism and clencing are habits increase occlusal loads and the increased horizontally directed heavy forces cause stress in bone implant connection. The loosening of proshtetic screws or multiunit abutment-implant connections or any fracture on temporary proshtesis may be early symptoms of any parafunctional habits (5). Low occlusal tubercle angles, narrow occlusal schemes, maximum symmetrical occlusal contacts distrubuted as much as possible should be aimed and distal cantilever should be avoided. If fracture of immediate prostehesis or frequent loosening of screws are observed, immediate loading protocol should be stopped and conventional healing period should be waited (6,7). In these cases, the use of a hard occlusal splint after delivery of the permanent prosthesis is recommended for minimizing the risks arising from occlusal overloads.

#4 Multiunit healing abutments and the appearance before permanent prosthesis
#5 The clinical appearance before placement of quattrofix implant system

#6 Placement of permanent quattrofix implant system prosthesis
Hasta Beklentileri
Gerçekçi olmayan hasta beklentilerini ortadan kaldırmak gerekir.
– Distal cantilever uzunluğu sağlam kemiğe sahip bireylerde 10-12 mm’i geçmemelidir. Yumuşak kemik kalitesine sahip bireylerde 6-8 mm cantilever yeterli görülmektedir. (5) Dolayısıyla genelde birinci büyükazı dişlerde biten bir protez uygulandığı için hastaların diş sayısı konusunda bilgilendirilmesi gerekmektedir. Geçici protezin 1. premolar seviyesinde biteceği belirtilmelidir.
– All-on-four protezlerinde doku ile protez arasında bir geçiş hattının olacağı ve bu hattın temizlenebilirliğin sağlanması amacıyla (ağız duşu, diş ipleri,vb..) hafif bir aralık bırakılacağı, kişinin bu açıklığı temizlediği sürece sorun yaşanmayacağı konusunda bilgi verilmeli ve oral hijyen motivasyonu sağlanmalıdır.
-Maliyet-fayda dengesi ve oklüzal kuvvetlerin derecesini ön görerek kullanılacak protezin materyali seçilmeli ve hastaya kullanılacak materyal alternatifleri anlatılmadır. (Bruksizm hastasında akrilik dişlerin seçimi gibi)
– Doğal dişlerde bruksizm alışkanlığı işareti olan bireylerde immediat yükleme sözü verilmemelidir. İmmediat yüklemede kayıplar çoğunlukla, normal sentrik oklüzyondaki kuvvetlerden dolayı değil, parafonksiyonel hareketler neticesinde olur.
– İmmediat yüklenen protezle yumuşak beslenilmesi önerilmektedir.

#7 Intraoral view of screw retained metal ceramic prosthesis

#8 Intraoral view of screw retained metal ceramic prosthesis
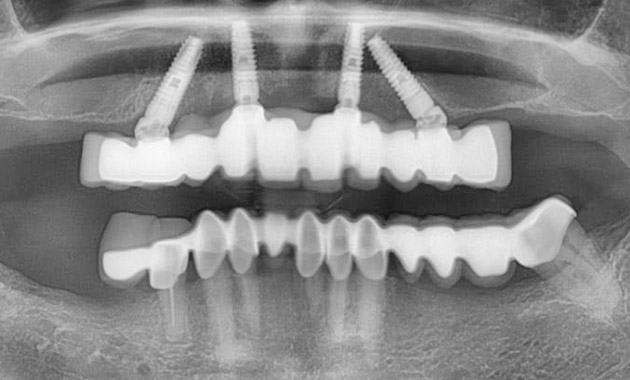
#9 Postoperative panoramic view